Neurosurgeon
SPINE | LAS VEGAS
Dr. Andrew Lee, MD | Nevada Spine Clinic, Las Vegas, Nevada
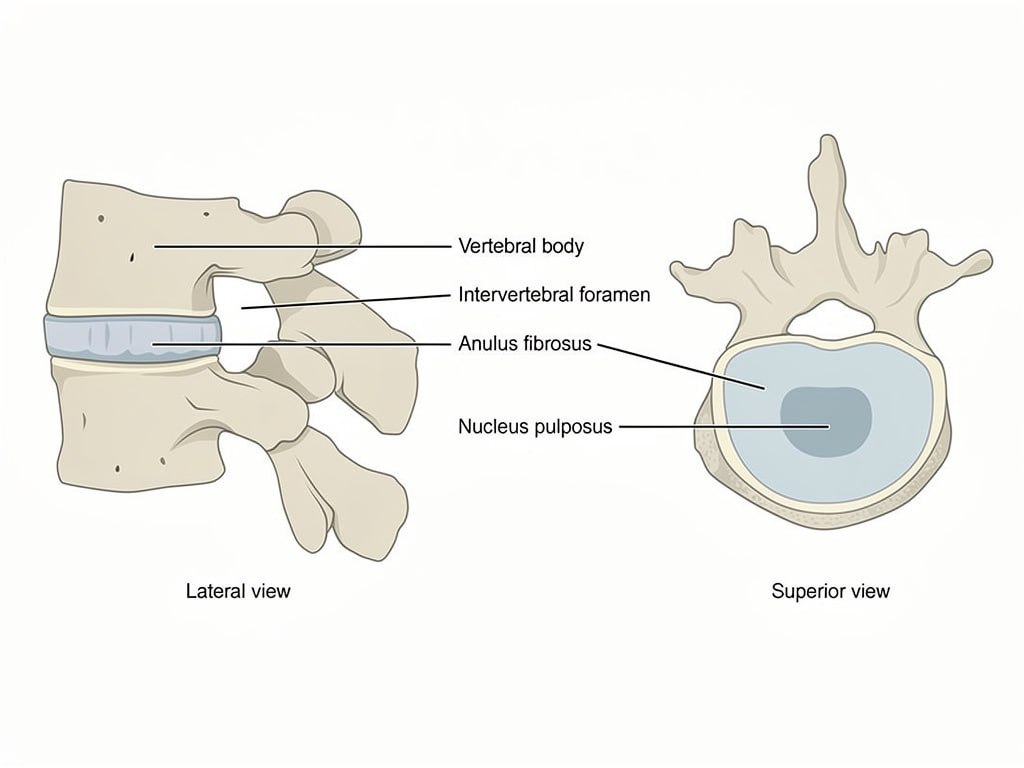
The lumbar spine consists of five vertebrae at the base of the back, supporting the majority of body weight. Between each vertebra lies an intervertebral disc that cushions load and allows movement. The lumbar spine also houses the nerve roots that travel down into the legs.
When lumbar discs degenerate or vertebrae slip out of alignment, nerve roots can become compressed, producing leg pain, numbness, or weakness. Dr. Andrew Lee at Nevada Spine Clinic in Las Vegas evaluates lumbar pathology carefully before recommending any surgical approach.
Dr. Andrew Lee at Nevada Spine Clinic in Las Vegas evaluates all lumbar fusion candidates for non-surgical options first. Physical therapy focused on core strengthening and lumbar stabilization, anti-inflammatory medications, and epidural steroid injections can provide meaningful relief for many patients.
Surgical intervention is considered only when symptoms have not responded to adequate conservative care or when progressive neurological signs are present.
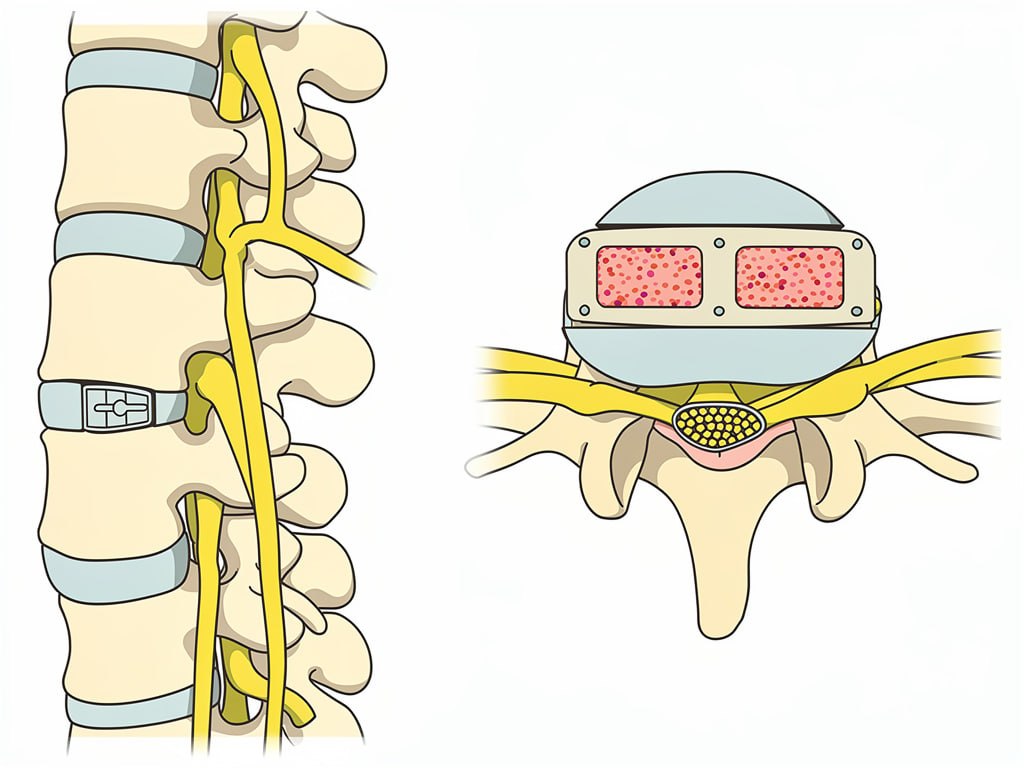
Lateral lumbar interbody fusion is a minimally invasive surgical approach that allows Dr. Andrew Lee to access the lumbar spine through a small incision on the patient’s side, completely avoiding the large back muscles. This approach significantly reduces tissue disruption compared to traditional posterior fusion techniques.
Dr. Lee performs LLIF at Southern Hills Hospital in Las Vegas using specialized instruments to work through the psoas muscle to reach the disc space from a lateral direction. The damaged disc is removed and a large interbody cage filled with bone graft material is placed in the disc space. This restores disc height, corrects alignment, and creates the conditions for bone fusion.
Posterior supplemental fixation with screws and rods is often added in a second step to provide rotational stability. The minimally invasive lateral approach results in less blood loss, shorter hospital stays, and faster recovery compared to open posterior approaches for many patients.
One of the advantages of the lateral approach is faster recovery compared to traditional open lumbar fusion. Most patients are walking the same day or the day after surgery. Dr. Lee encourages early mobilization to promote healing and reduce complications.
A lumbar brace may be prescribed for several weeks. Physical therapy focused on core stabilization is typically started four to six weeks after surgery. Full recovery and return to unrestricted activity generally occurs between three and six months.
Leg pain and radicular symptoms often improve quickly as nerve root pressure is relieved by the restoration of disc height. Lower back pain improvement may be more gradual as the fusion heals.
Temporary thigh numbness or hip flexor weakness on the approach side is common and resolves in the majority of patients within weeks to months.
Patients should not drive until Dr. Lee provides specific clearance at follow-up.
No bathtub, swimming, or hot tub until cleared by Dr. Lee.
The lateral incision is typically small and heals quickly. Avoid soaking the wound in water until cleared by Dr. Lee. Follow showering instructions provided at discharge.
Pain medications should be taken as prescribed. For refills, contact your pharmacy at least forty-eight hours in advance. Refills are not processed on weekends or after office hours.
Wear the lumbar brace as instructed during the early recovery period. Avoid bending, twisting, and lifting beyond prescribed limits until Dr. Lee clears progressive
activity.
Walking is the most important early activity. Begin with short frequent walks and gradually increase duration over the first six weeks. Contact Nevada Spine Clinic or go to the emergency room for sudden neurological changes, fever, or significantly worsening pain.
No bathtub, swimming, or hot tub until cleared by Dr. Lee.
Dr. Andrew Lee, MD | Nevada Spine Clinic, Las Vegas
Your information is private and will never be shared.