Neurosurgeon
SPINE | LAS VEGAS
Dr. Andrew Lee, MD | Nevada Spine Clinic, Las Vegas, Nevada
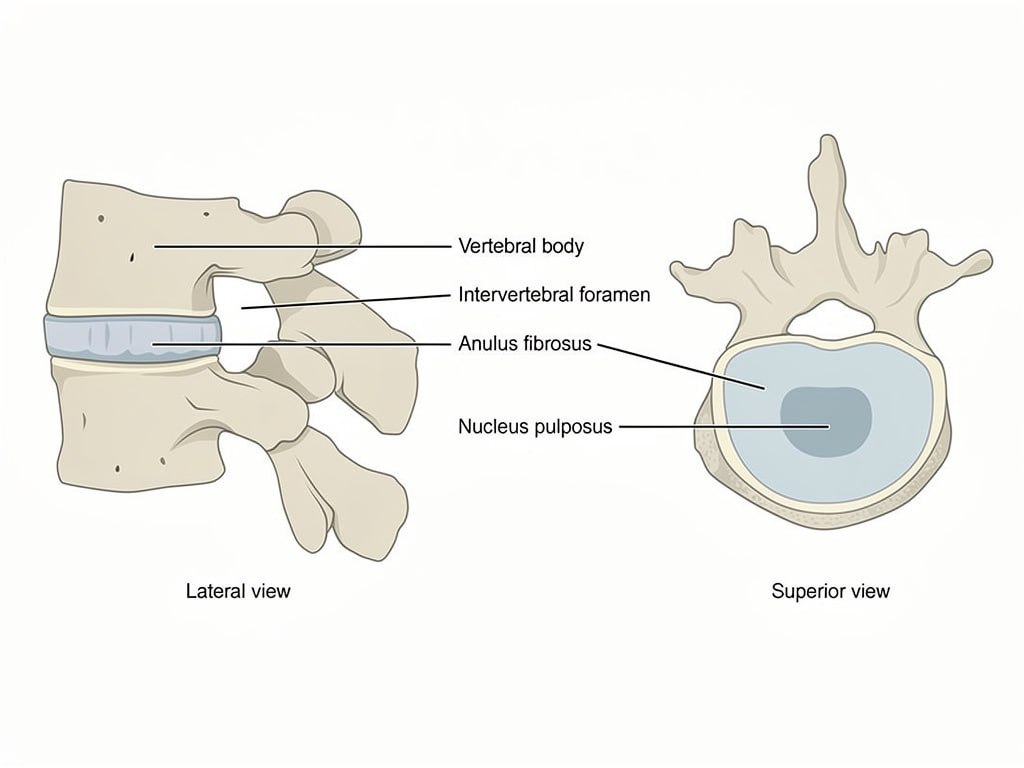
The lumbar spine consists of five vertebrae that bear the majority of the body’s weight and allow the trunk to bend, extend, and rotate. Between each pair of vertebrae lies an intervertebral disc that acts as a shock absorber and pivot point. When lumbar discs degenerate, the loss of disc height and hydration reduces their ability to absorb load and can compress the nerve roots that exit the spine.
Dr. Andrew Lee at Nevada Spine Clinic in Las Vegas evaluates each patient’s anatomy, symptoms, and activity goals before recommending any surgical treatment.
Before considering lumbar ADR, Dr. Andrew Lee at Nevada Spine Clinic in Las Vegas ensures patients have had an adequate course of conservative treatment. This includes physical therapy with core strengthening, anti-inflammatory medications, activity modification, and lumbar epidural steroid injections when appropriate.
Lumbar ADR is considered only after a minimum of six months of conservative care without adequate improvement, in patients with appropriate anatomy and without significant instability or osteoporosis.
Anterior lumbar artificial disc replacement offers patients with lumbar disc disease a motion-preserving alternative to fusion. Dr. Andrew Lee performs lumbar ADR at Southern Hills Hospital in Las Vegas for carefully selected patients with one or two level degenerative disc disease.
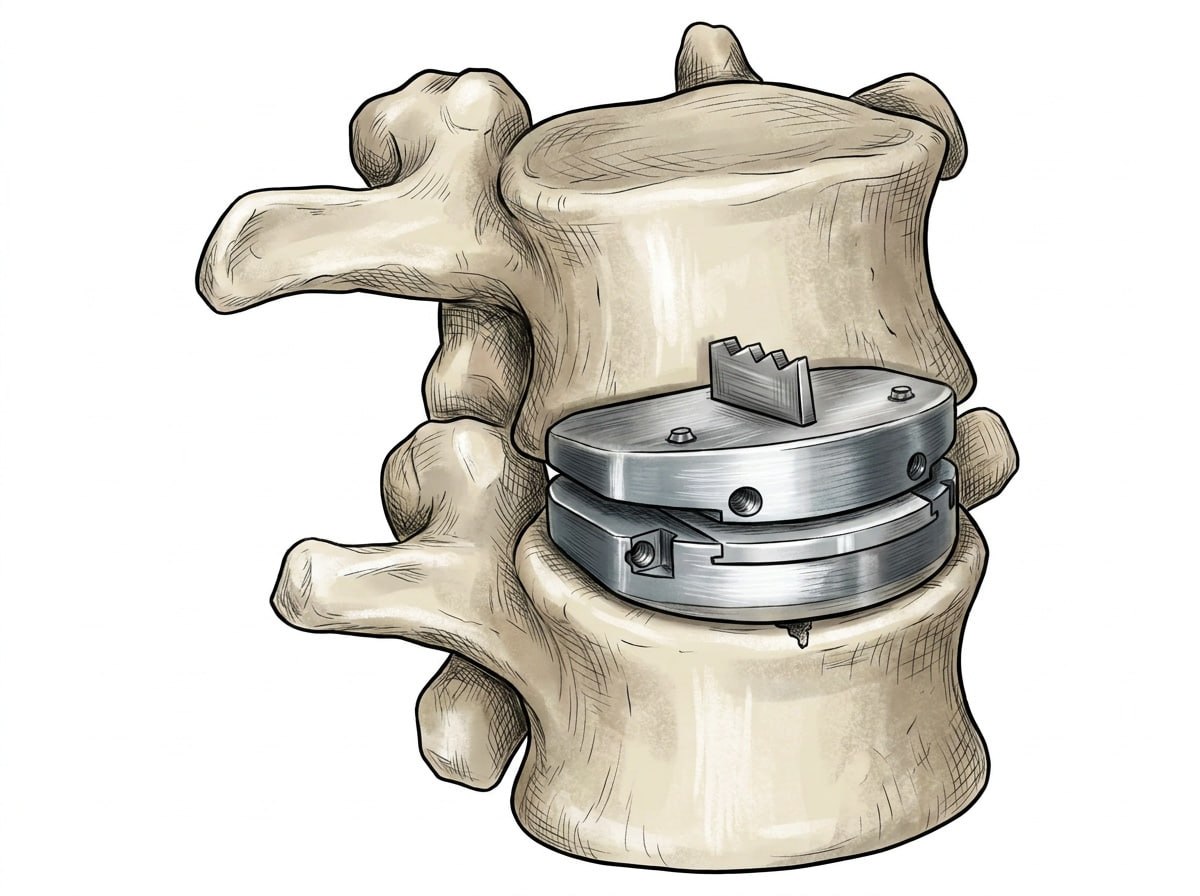
The procedure is performed through an anterior abdominal incision, accessing the lumbar spine from the front with the assistance of a vascular surgeon to safely mobilize the major blood vessels. The degenerated disc is completely removed and an artificial disc prosthesis is implanted in the disc space. The device replicates the natural motion of a healthy lumbar disc, maintaining flexibility and load distribution at the treated level.
By preserving motion, lumbar ADR avoids the adjacent segment stress that fusion imposes on neighboring discs. Patients who qualify can expect a faster return to activity and maintained lumbar flexibility compared to fusion.
Recovery following lumbar ADR is generally faster than lumbar fusion. Most patients are walking on the day of surgery or the following morning. Dr. Lee encourages early gentle movement to promote recovery.
Physical therapy focusing on core stabilization and lumbar mobility is typically introduced four to six weeks after surgery. Most patients return to light activity within four to eight weeks and full activity within three to six months.
Relief of discogenic lower back pain following lumbar ADR is typically experienced within the first few weeks as post-operative inflammation resolves. Preserved lumbar motion allows patients to return to activities that fusion would restrict.
Some abdominal muscle weakness or stiffness is expected in the early weeks following surgery and resolves with rehabilitation. Patients should not drive until Dr. Lee provides clearance at their follow-up visit.
No bathtub, swimming, or hot tub until cleared by Dr. Lee.
Pat the incision dry after showering and apply a clean dry bandage. Contact Nevada Spine Clinic if you notice increasing redness, warmth, swelling, or drainage from the incision site.
Pain medications may cause constipation. Maintain adequate hydration and fiber intake and continue your walking program. Prescription refills require forty-eight hours notice and are not processed on weekends or after business hours.
Avoid heavy lifting, bending, and twisting during the early recovery period. Walking is encouraged and increased gradually over the first six weeks. Driving is not permitted until Dr. Lee provides specific clearance.
Contact Nevada Spine Clinic immediately or go to the nearest emergency room if you experience sudden leg weakness, loss of bladder or bowel control, fever above 101.5 degrees Fahrenheit, or increasing abdominal pain.
No bathtub, swimming, or hot tub until cleared by Dr. Lee.
Dr. Andrew Lee, MD | Nevada Spine Clinic, Las Vegas
Your information is private and will never be shared.