Understanding the Cervical Spine
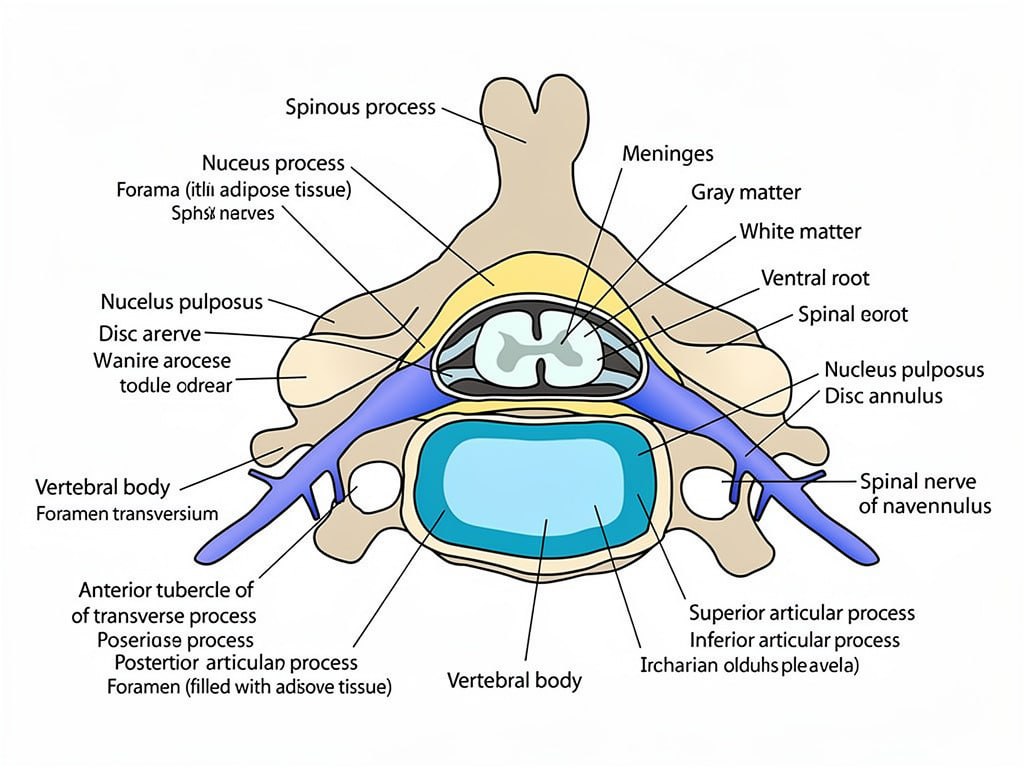
The cervical spine is made up of seven vertebrae stacked vertically in the neck. Between each vertebra lies an intervertebral disc that acts as both a cushion and a joint, allowing the neck to move in multiple directions while protecting the spinal cord and nerve roots. Each disc has a firm outer layer called the annulus fibrosus and a soft gel-like center called the nucleus pulposus.
When a cervical disc degenerates or herniates, it can compress nearby nerve roots or the spinal cord, producing pain, numbness, tingling, or weakness that radiates into the arms and hands. Dr. Andrew Lee at Nevada Spine Clinic in Las Vegas evaluates each patient carefully to determine the most appropriate treatment for their specific anatomy and symptoms.
Common Cervical Spine Conditions
Herniated Disc: When the inner gel-like material of a cervical disc pushes through its
outer wall, it can compress nearby nerves and cause radiating arm pain,
numbness, tingling, or weakness.
Degenerative Disc Disease: With age, cervical discs lose moisture, height, and structural integrity. This progressive degeneration can lead to nerve compression, chronic neck
pain, and stiffness.
Cervical Stenosis: Narrowing of the spinal canal in the neck compresses the spinal cord or nerve roots. Severe cases can cause balance difficulties, weakness, and
changes in bowel or bladder function.
Cervical Instability: Some patients develop abnormal movement between cervical vertebrae due to disc or ligament deterioration, requiring surgical stabilization to protect the spinal cord.
Conservative Non-Surgical Care
Before recommending surgery, Dr. Andrew Lee at Nevada Spine Clinic in Las Vegas explores all appropriate non-surgical options. Conservative treatment for cervical disc conditions typically includes anti-inflammatory medications to reduce nerve swelling, physical therapy focused on posture correction and neck strengthening, and cervical traction to relieve disc pressure.
Corticosteroid injections delivered near the affected nerve root can provide meaningful temporary relief. Surgery is recommended only when symptoms have not responded adequately to conservative care or when neurological signs are progressing.
Anterior Cervical Discectomy and Fusion
Anterior cervical discectomy and fusion, commonly referred to as ACDF, is one of th most well-established procedures in spine surgery. Dr. Andrew Lee performs ACDF Southern Hills Hospital in Las Vegas for patients whose cervical disc disease has not responded to conservative care and who are not candidates for motion-preservin disc replacement.
The procedure involves making a small incision in the front of the neck to access the cervical spine. The damaged or herniated disc is carefully removed to relieve pressure from the spinal cord and nerve roots. A bone graft or interbody spacer is then placed in the disc space to maintain proper vertebral height and alignment. A small titanium plate and screws are applied to stabilize the segment and promote bone fusion.
Over time, the adjacent vertebrae grow together to form a solid fused segment, eliminating motion at that level. ACDF has a long track record of effectiveness and is appropriate for patients with instability, multilevel disease, or anatomy that makes disc replacement unsuitable.
The primary goals of this procedure are to:
Relieve pressure on the spinal cord and nerve roots
Eliminate pain, numbness, and weakness caused by disc compression • Stabilize the cervical spine and restore proper alignment
Prevent further neurological deterioration
Potential Risks
Nerve or spinal cord injury: Rare but possible. May result in temporary or permanent changes in strength, sensation, or coordination.
Dural tear: Accidental disruption of the membrane surrounding the spinal cord may
cause spinal fluid leakage requiring additional treatment.
Infection: Superficial or deep infections can occur. Preventive antibiotics are given and proper wound care is essential during recovery.
Breathing difficulties: Rare swelling in the neck can affect the airway. Seek emergency care immediately if breathing is compromised after discharge.
Adjacent segment disease: Fusion eliminates motion at the treated level, which may over time increase stress on the discs above and below.
Other complications: Voice hoarseness, swallowing difficulties, blood clots, or pneumonia may occur. Most resolve without further intervention.
Anterior cervical discectomy and fusion, commonly referred to as ACDF, is one of th most well-established procedures in spine surgery. Dr. Andrew Lee performs ACDF Southern Hills Hospital in Las Vegas for patients whose cervical disc disease has not responded to conservative care and who are not candidates for motion-preservin disc replacement.
Postoperative Recovery and Rehabilitation
Recovery following ACDF begins on the day of surgery. Dr. Lee encourages early walking to promote circulation and reduce the risk of complications. Most patients walk for fifteen minutes twice daily by their first follow-up appointment. By six weeks the goal is thirty to forty minutes of walking twice daily.
Neck strengthening exercises are introduced gradually as comfort allows. Gentle range of motion is permitted but forced bending, twisting, and heavy lifting should be avoided during the early recovery period.
What to Expect After Surgery
Relief of arm symptoms including pain, numbness, and tingling is often experienced immediately or within the first few days following surgery. If nerve compression has been present for an extended period, nerve healing may take weeks to months.
Muscle strength typically recovers before numbness resolves. Numbness that existed for many months before surgery may take longer to improve and in some cases may be permanent.
Incision discomfort generally improves significantly within two to three weeks. Patients are advised not to drive for approximately three weeks or until cleared by Dr. Lee at their follow-up visit.
Do not soak your wound.
No bathtub, swimming, or hot tub until cleared by Dr. Lee.
Wound Care and Medication Management
Your incision will be evaluated at the first post-operative visit and sutures removed if necessary. Avoid soaking the wound in water, including baths, hot tubs, and swimming, until cleared by Dr. Lee.
If a clear plastic dressing covers the wound, you may remove it at home and shower immediately. If a gauze dressing is in place, wait seventy-two hours before showering and only if the dressing is dry. Pat the incision dry after showering and apply a clean dry bandage.
Pain medications may cause constipation. Increase fluid intake, eat plenty of fruits and vegetables, and maintain your walking routine. For prescription refills contact your pharmacy with at least forty-eight hours notice.
Activity Guidelines After Surgery
Avoid extreme forward or backward bending of the neck and do not twist the neck to its limits during recovery. Gentle neck movement within comfortable range is acceptable and encouraged. Do not resume driving until Dr. Lee has cleared you at your follow-up appointment.
Contact Nevada Spine Clinic immediately or go to the nearest emergency room if you develop difficulty breathing, a temperature above 101.5 degrees Fahrenheit, sudden weakness or balance changes, or pain that is significantly worsening.