Neurosurgeon
SPINE | LAS VEGAS
Dr. Andrew Lee, MD | Nevada Spine Clinic, Las Vegas, Nevada
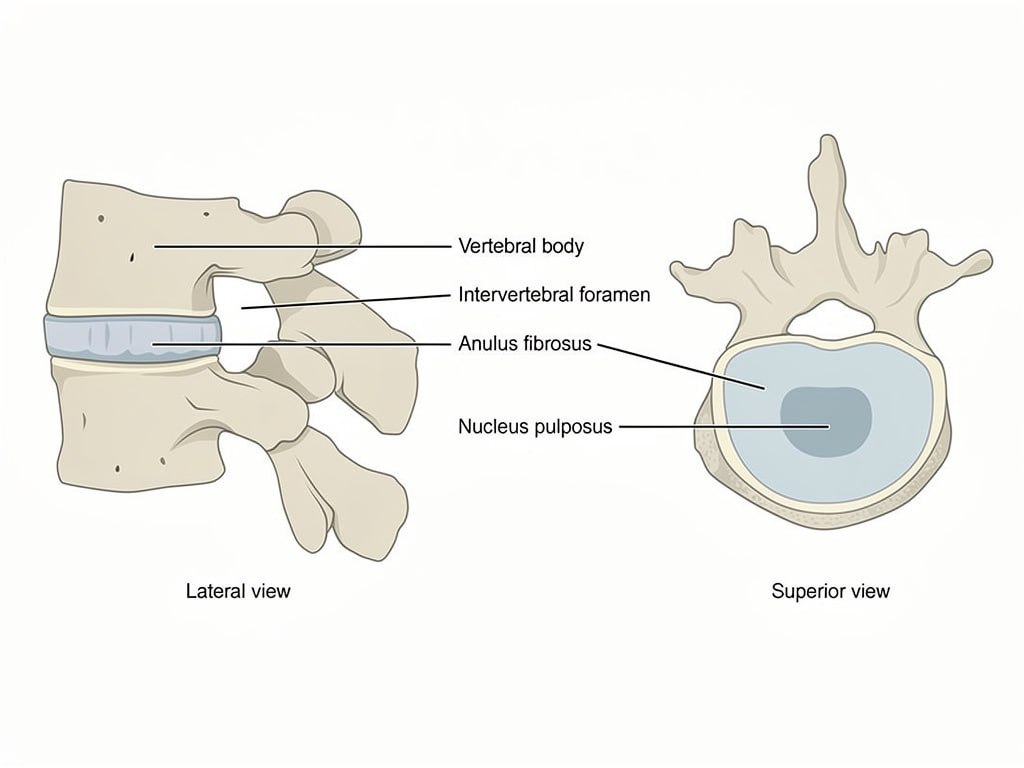
The lumbar spine bears the majority of the body’s mechanical load and allows the trunk to bend, extend, and rotate. The intervertebral discs between the five lumbar vertebrae distribute this load and provide flexibility. When discs degenerate or vertebrae become unstable, surgical stabilization through fusion may be necessary.
The anterior approach to the lumbar spine allows Dr. Andrew Lee to place a larger interbody graft than posterior approaches permit, improving fusion rates and restoring disc height more effectively in appropriate patients.
Dr. Andrew Lee at Nevada Spine Clinic in Las Vegas ensures all candidates for lumbar fusion have completed an adequate course of conservative management including physical therapy, medications, and injections before surgical intervention is recommended.
ALIF is reserved for patients in whom non-operative treatment has failed and in whom the anatomy and clinical findings support the anterior approach as the most appropriate surgical strategy.
Anterior lumbar interbody fusion allows Dr. Andrew Lee to access the lumbar spine through an incision in the lower abdomen, reaching the front of the disc space directly. This procedure is performed at Southern Hills Hospital in Las Vegas with vascular surgery assistance to safely mobilize the aorta and vena cava.
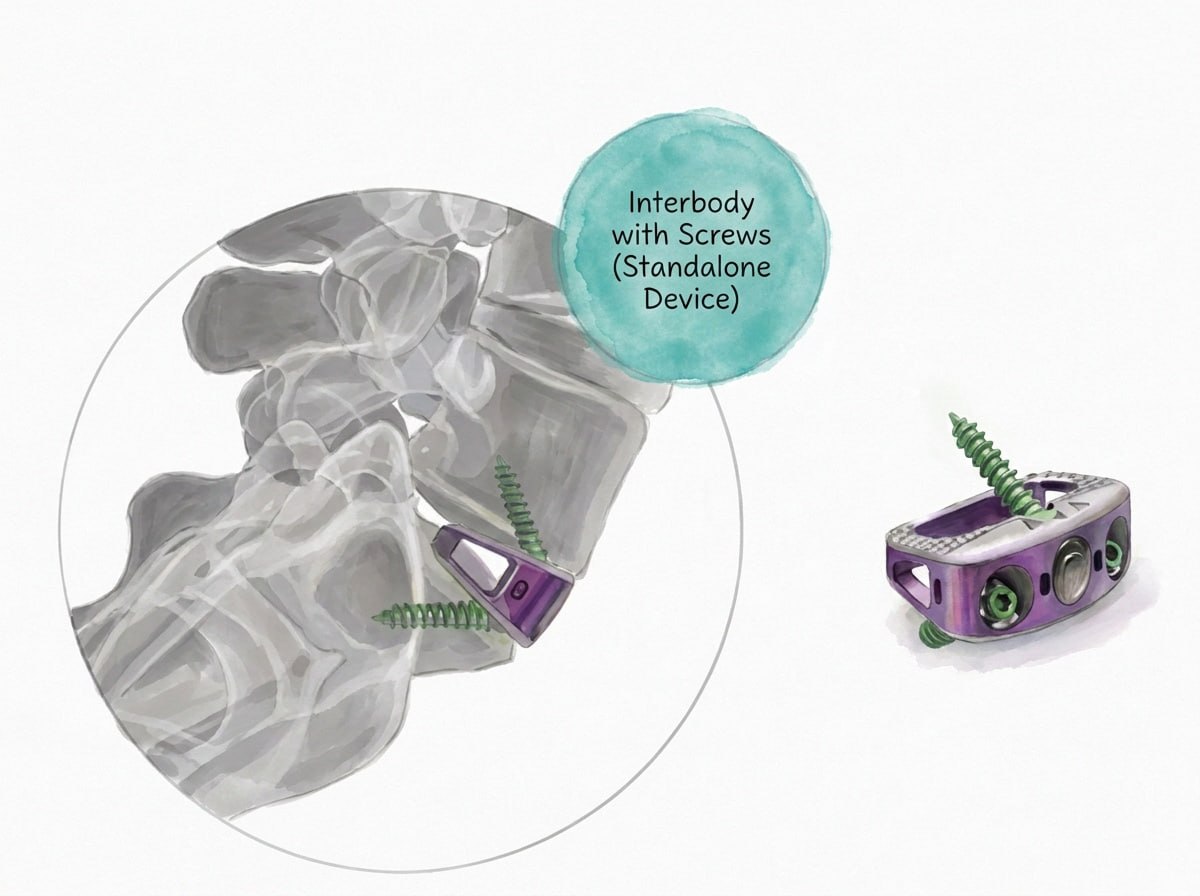
The degenerated disc is completely removed and a large interbody cage packed with bone graft material is placed in the disc space. The larger footprint of an anterior cage compared to posterior approaches allows for better restoration of disc height, lumbar lordosis, and endplate contact area, all of which contribute to higher fusion rates.
Posterior percutaneous screw fixation is typically added through separate small incisions to provide rotational stability. ALIF is particularly effective for restoring lumbar alignment and is a component of many complex lumbar reconstruction procedures.
Most patients undergoing ALIF are hospitalized for one to two nights. Walking begins the day of or day after surgery. A lumbar brace is typically worn for several weeks to protect the reconstruction during early healing.
Physical therapy is introduced at four to six weeks focusing on core strengthening and gradual return to activity. Most patients return to light work within four to six weeks and full activity within four to six months.
Lower back pain improvement is typically gradual as the fusion consolidates over three to six months. Leg pain from nerve compression often improves more quickly as the nerve root decompression takes effect.
Some temporary abdominal muscle weakness and stiffness following the anterior approach is expected and improves with rehabilitation over several weeks.
No bathtub, swimming, or hot tub until cleared by Dr. Lee.
Follow wound care instructions provided at discharge. Avoid soaking the incision in water until cleared by Dr. Lee. The abdominal incision requires careful monitoring for signs of infection during healing.
Maintain adequate hydration and nutrition to support fusion healing. Pain medication refills require forty-eight hours notice from your pharmacy and are not processed on weekends.
Wear the prescribed lumbar brace as directed. Avoid heavy lifting, bending, and twisting during the early recovery period. Do not drive until Dr. Lee provides clearance at your follow-up appointment.
Contact Nevada Spine Clinic or the nearest emergency room immediately for sudden neurological changes, abdominal pain, fever above 101.5 degrees Fahrenheit, or significant wound changes.
No bathtub, swimming, or hot tub until cleared by Dr. Lee.
Dr. Andrew Lee, MD | Nevada Spine Clinic, Las Vegas
Your information is private and will never be shared.