Neurosurgeon
SPINE | LAS VEGAS
Dr. Andrew Lee, MD | Nevada Spine Clinic, Las Vegas, Nevada
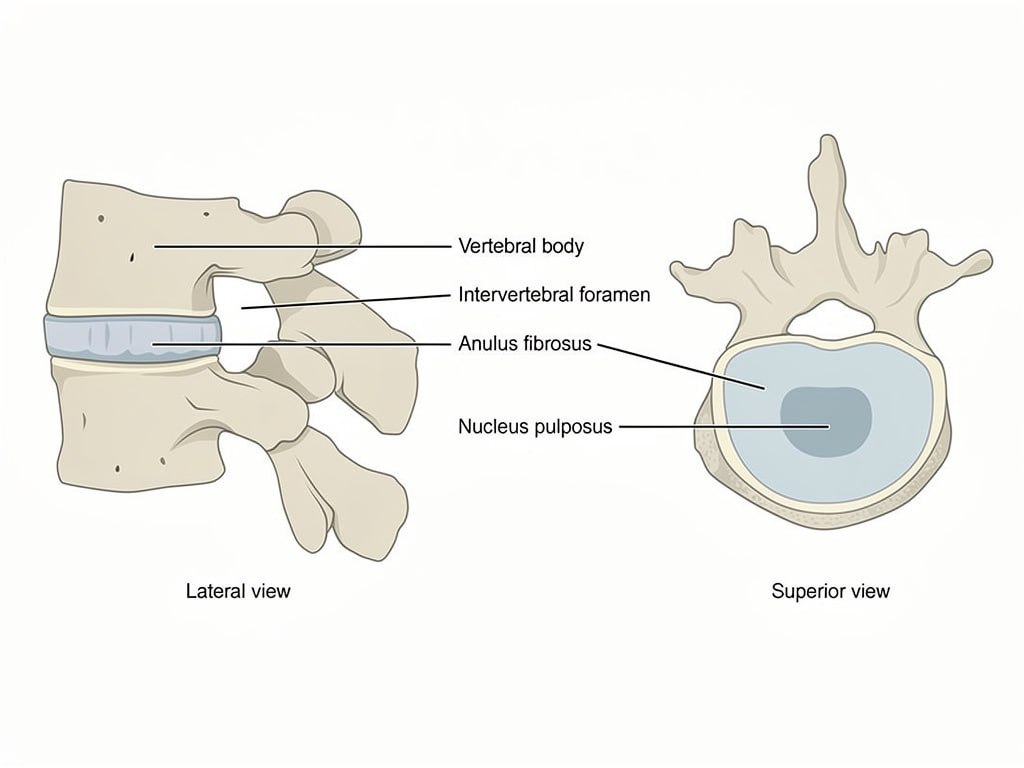
The lumbar spine provides structural support for the upper body and houses the nerve roots that supply the legs and feet. Stability between vertebrae depends on healthy discs, intact facet joints, and surrounding musculature. When these structures fail due to degeneration, injury, or prior surgery, pedicle screw fixation provides reliable stabilization.
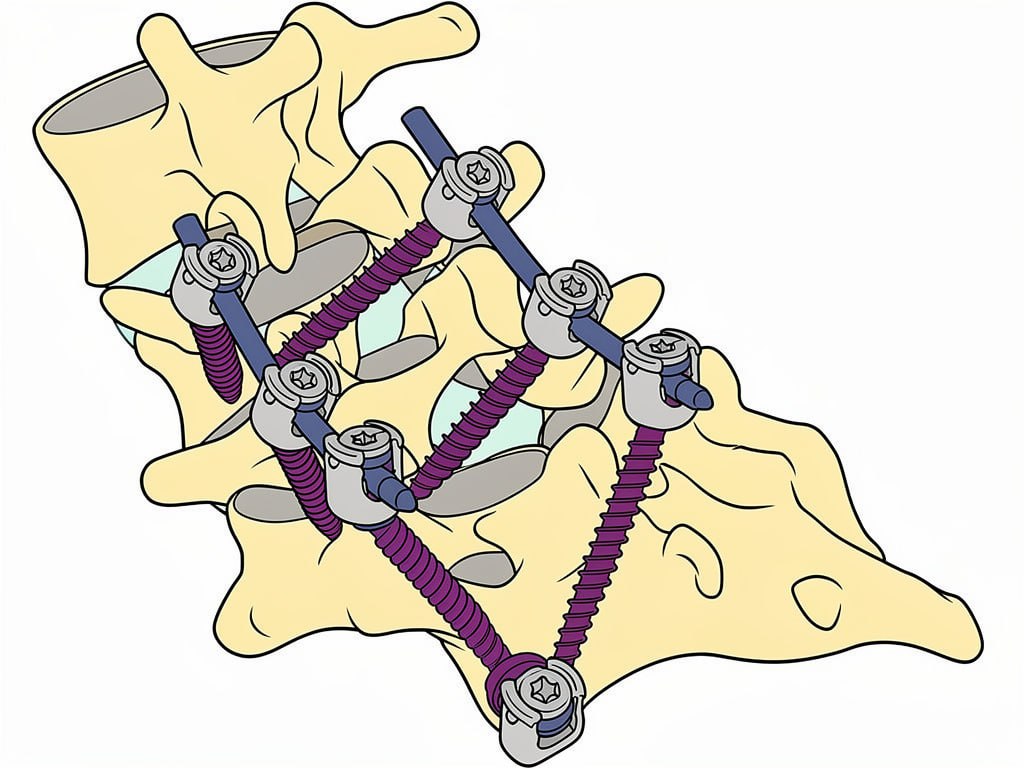
Pedicle screws are placed through the strongest bony structure of each vertebra, the pedicle, which connects the posterior arch to the vertebral body. This allows forces to be distributed effectively through the implant and facilitates bone fusion across the treated segments.
Dr. Andrew Lee at Nevada Spine Clinic in Las Vegas exhausts appropriate conservative measures before recommending posterior spinal fusion. Physical therapy, medications, injections, and activity modification are all evaluated.
Posterior fusion with pedicle screws is recommended when non-operative care has failed and imaging confirms the structural pathology correlates with the patient’s symptoms.
Posterior spinal fusion with pedicle screws is one of the most commonly performed lumbar fusion procedures and has a well-established record of clinical success. Dr. Andrew Lee performs this procedure at Southern Hills Hospital in Las Vegas using techniques designed to maximize fusion rates while minimizing muscle disruption.
Through a posterior midline incision, Dr. Lee places pedicle screws bilaterally at each level to be fused. Titanium rods connect the screws to create a rigid construct. Bone graft is placed along the decorticated posterior elements to promote biological fusion. In many cases an interbody cage is also placed through the posterior approach to provide anterior column support.
Pedicle screw fixation holds the vertebrae in proper alignment while the bone graft heals and fuses across the treated segments, typically over three to six months.
Walking begins on the day of or day after surgery. Most patients are discharged after one to two nights in hospital. A lumbar brace is typically worn for six to eight weeks while the fusion consolidates.
Physical therapy begins at four to six weeks focusing on core strengthening, gait training, and gradual return to function. Most patients return to light activity at six to eight weeks and full activity at three to six months.
Leg pain from nerve compression often improves quickly following decompression. Lower back pain improvement is more gradual, typically occurring over three to six months as the fusion heals.
Posterior lumbar surgery involves dissection of the back muscles, which causes some post-operative back stiffness and soreness that improves with rehabilitation over several months.
No bathtub, swimming, or hot tub until cleared by Dr. Lee.
The posterior lumbar incision requires careful wound care during healing. Avoid soaking the wound until cleared by Dr. Lee. Follow the specific showering and dressing instructions provided at discharge.
Monitor the incision for increasing redness, warmth, swelling, or drainage. Contact Nevada Spine Clinic promptly if any of these signs develop. Prescription refills require forty-eight hours advance notice.
Wear the lumbar brace as prescribed during the recovery period. Avoid heavy lifting, bending, and twisting. Walking daily is encouraged and is the most important early activity.
Do not drive until Dr. Lee provides clearance. Contact Nevada Spine Clinic or go to the nearest emergency room immediately for sudden leg weakness, loss of bladder or bowel control, fever, or significant wound changes.
No bathtub, swimming, or hot tub until cleared by Dr. Lee.
Dr. Andrew Lee, MD | Nevada Spine Clinic, Las Vegas
Your information is private and will never be shared.